Introduction
If your hospital already runs a HIMS — Hospital Information Management System — you may be wondering whether you really need a separate paperless IPD solution. It’s a fair question.
The honest answer is that most HIMS platforms manage hospital operations well: OPD scheduling, pharmacy, lab reports, and billing modules. But the IPD documentation layer — the actual clinical records generated at the bedside, ward by ward, shift by shift — is where most HIMS solutions fall short.
And that gap between your HIMS and your IPD documentation is where billing errors happen, revenue leaks, and discharge processes break down.
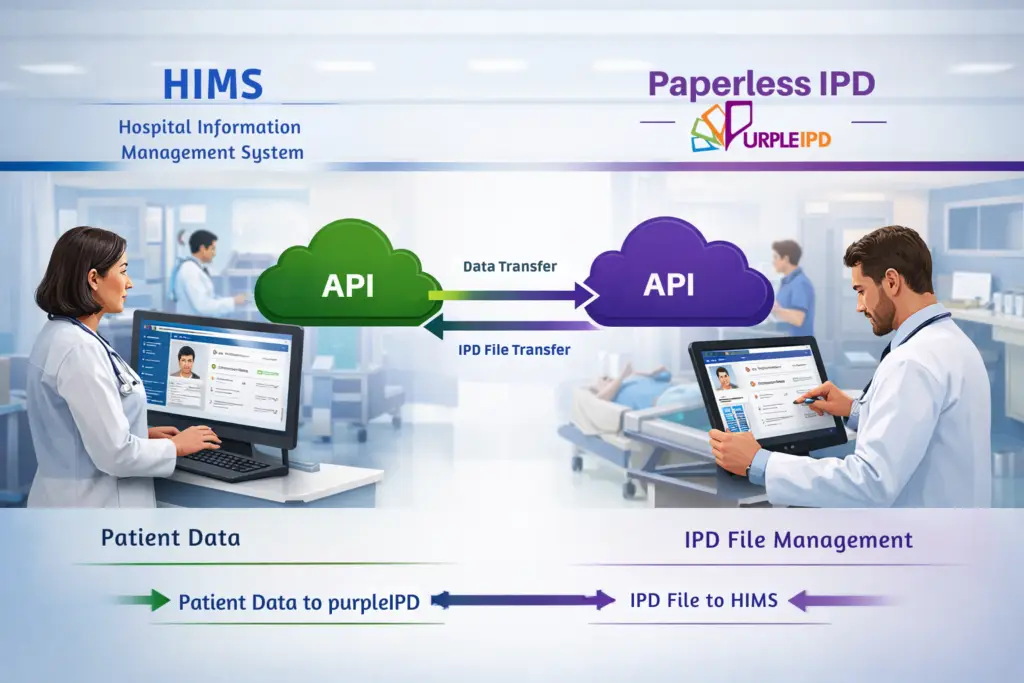
PurpleIPD doesn’t replace your HIMS. It integrates with it — filling exactly that gap, and connecting both systems so that patient data flows seamlessly from admission to discharge to billing without manual re-entry, file discrepancies, or post-discharge corrections.
The Problem: Two Systems That Don’t Talk to Each Other
In most Indian hospitals running a HIMS today, here is what actually happens at the ward level:
The HIMS records the patient’s admission, bed assignment, and billing information. The IPD documentation — nursing notes, doctor orders, medication charts, investigation requests, consent forms — is managed separately, often still on paper or in a disconnected digital system.
When it is time for discharge, the billing team generates an invoice from the HIMS. But the IPD file — still being updated by clinical staff — may not reflect the final picture. Procedures get added after billing. Medications are recorded late. A label change on a bed or ward doesn’t reflect in the IPD file. The bill goes out based on incomplete information.
The result: billing errors, revenue leakage, disputes with patients, and IPD files that keep getting modified after the invoice has already been raised.
A well-integrated HIMS should manage all aspects of a hospital’s operations, including medical, financial, administrative, legal, and compliance functions — but only Purpleipd when the IPD documentation layer is properly connected to it.
How PurpleIPD Integrates With Your Existing HIMS
PurpleIPD is built to work alongside your existing HIMS — not replace it. We have partnered with multiple HIMS providers and built co-sell partnerships specifically so hospitals get a seamless, integrated experience from day one without disrupting existing workflows.
Here is what the integration actually enables:
Patient information flows automatically: When a patient is admitted and registered in your HIMS, their demographic information, insurance details, and bed assignment flow directly into their PurpleIPD record. No duplicate data entry. No risk of name mismatches or missing patient IDs between systems.
Bed and ward transfers reflect instantly: When a patient is transferred from a general ward to ICU — or from one bed to another — the change is reflected immediately in the IPD file. Clinical staff always see the current location. Nursing assignments, medication charts, and ward-specific documentation update automatically. Label changes at the ward level are handled automatically.
Discharge only happens when the IPD file is closed: This is the most commercially significant integration point. PurpleIPD locks the IPD file for editing before discharge is permitted. Once the treating doctor closes the IPD record — confirming that all documentation is complete, all procedures are recorded, and all forms are signed off — only then does the system allow discharge to proceed and the billing module in your HIMS to generate the final invoice.
This single mechanism eliminates an entire category of billing errors that most hospitals accept as unavoidable: procedures recorded after billing, medications added post-discharge, and IPD files modified after invoices have been raised.
The Revenue Leakage Problem — and How Integration Solves It
Revenue leakage in Indian hospitals is rarely caused by fraud. It is almost always caused by process gaps — specifically, the gap between what was actually done for a patient and what was captured in the billing system before the invoice was generated.
A surgeon adds a procedure note after the patient has already been billed. A nurse records a consumable after discharge. A medication is administered but never entered into the IPD file before it was closed for billing. In each case, the hospital has incurred a cost that it cannot recover because the invoice has already been raised.
Hospital management software helps automate processes and reduce the burden on staff and doctors — but only PurpleIPD when the IPD documentation and billing systems are properly connected with the right controls in place.
PurpleIPD’s discharge lock mechanism makes this gap structurally impossible. The IPD file cannot be modified after it is closed. The discharge cannot be triggered before the file is closed. The sequence is enforced by the system — not by staff discipline or manual checks.
For a hospital processing 200 IPD cases a month, plugging even small per-case revenue leakage compounds into significant monthly revenue recovery.
Reducing Billing Errors — The Three Biggest Sources
1. Post-discharge IPD file modifications: Without a discharge lock, clinical staff can and do update IPD files after patients leave. These late entries never make it into the bill. With PurpleIPD’s HIMS integration, the file is locked at the point of discharge authorisation — no modifications are possible after billing is triggered.
2. Bed and ward transfer mismatches: When a patient moves wards mid-admission, their billing classification often changes — ICU rates differ from general ward rates. If the HIMS doesn’t receive the transfer signal from the IPD system in real time, the wrong rate gets applied. PurpleIPD’s integration ensures every bed and ward transfer updates both systems simultaneously.
3. Duplicate and manual data entry errors: In a disconnected system, patient information entered into the HIMS at admission gets re-entered manually into the IPD documentation system. Every manual re-entry is an opportunity for error — wrong patient ID, wrong diagnosis code, wrong insurance details. With PurpleIPD’s HIMS integration, data entered once in either system populates both — eliminating the entire category of duplication errors.
Which HIMS Systems Does PurpleIPD Integrate With?
PurpleIPD has established integration partnerships with multiple leading HIMS providers used across Indian hospitals. Our co-sell partnerships mean that when your hospital implements PurpleIPD alongside your existing HIMS, both vendors work together to configure the integration — you don’t manage two separate vendor relationships or coordinate the technical setup yourself.
If your hospital is currently evaluating HIMS options alongside a paperless IPD solution, our team can advise on which combinations deliver the most seamless integration for your specific workflows and compliance requirements.
Contact us to discuss your hospital’s current HIMS setup and we will walk you through exactly how PurpleIPD integrates with your existing system.
Conclusion
Your HIMS is an essential foundation. But the IPD documentation layer — where clinical records are generated, procedures are captured, and billing accuracy is determined — requires a dedicated solution that connects to your HIMS rather than sitting beside it as a separate silo.
PurpleIPD’s HIMS integration closes that gap: patient data flows without re-entry, bed transfers update both systems in real time, and the discharge lock ensures billing only happens on complete, locked IPD records.
The result is fewer billing errors, less revenue leakage, and a controlled, compliant, and commercially accurate discharge process.
To see how PurpleIPD integrates with your specific HIMS setup, book a 20-minute demo.