The Two Layers of Hospital Management Software in India
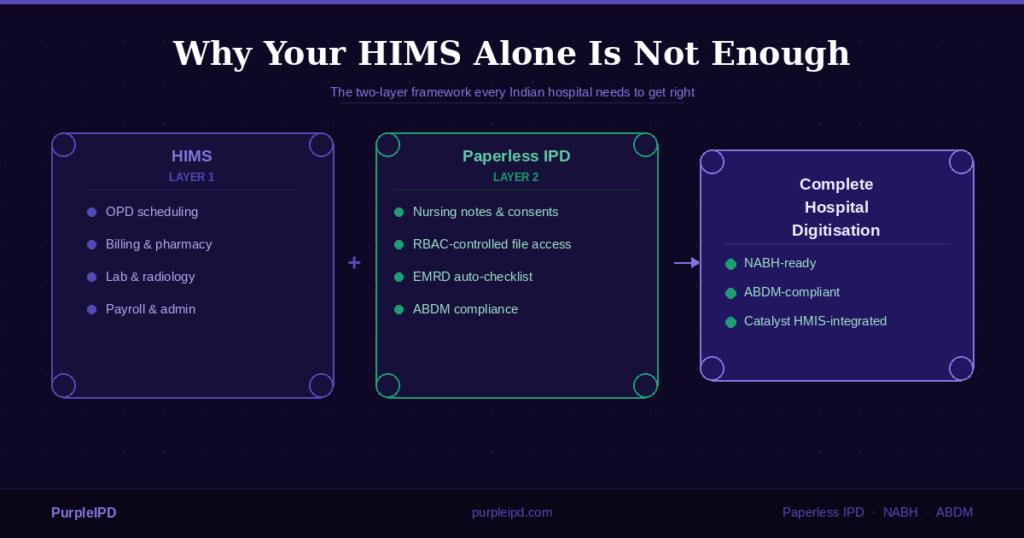
Most people use the term “HMS” to mean everything a hospital needs to run digitally. In practice, however, hospital software spans two fundamentally different operational layers — each serving different staff, compliance requirements, and workflows.
Layer 1 — HIMS / Operational
- OPD scheduling and registration
- Billing, insurance, and claims
- Pharmacy and lab management
- Payroll and administration
- Financial reporting and MIS
Layer 2 — IPD Documentation / Clinical
- Nursing notes and doctor orders
- Medication charts and consent forms
- EMRD checklists and discharge summaries
- RBAC-controlled file access
- ABDM-compliant records at source
Most established HIMS platforms in India handle Layer 1 reliably. Consequently, however, almost none handle Layer 2 with the clinical depth, bedside usability, and compliance controls that NABH-accredited and ABDM-compliant hospitals require. Therefore, hospitals that invest only in a HIMS are — knowingly or not — leaving Layer 2 to paper.
The key insight: When hospital administrators report billing discrepancies, discharge delays, or NABH audit failures, the root cause is almost always in Layer 2 — not Layer 1. Solving the wrong layer costs time and money without fixing the problem.
What HIMS Does Well — And Where It Was Designed to Stop
A well-implemented Hospital Information Management System is the operational backbone of any modern hospital. It creates a single source of truth for patient registration, financial transactions, inventory, and clinical reporting. These systems have matured significantly in India over the last decade and deserve their central role in hospital IT infrastructure.
However, HIMS platforms were architecturally designed for structured, predictable workflows. A billing transaction follows a defined sequence. A lab report has a fixed format. A pharmacy dispense is recorded at one point in time by one user.
IPD documentation does not work like this. Specifically, the clinical layer is chaotic, shift-dependent, and asynchronous. A nursing note gets updated at 3 AM. A consent form is added mid-admission when a procedure changes. A doctor’s order is written retrospectively. Importantly, none of this happens at a desk — it happens at the bedside, between clinical tasks, by staff who need speed, not software complexity.
No HIMS was designed to manage that environment. Accordingly, expecting it to be the source of most IPD documentation failures in Indian hospitals today.
For hospitals that need a complete solution, the most effective stack combines a proven HIMS with dedicated paperless IPD software — and in India specifically, that combination needs to be ABDM-compliant and NABH-ready from day one.
The IPD Documentation Layer: What It Is and Why It Is Different
The IPD documentation layer encompasses every clinical record generated during a patient’s inpatient stay — from admission to discharge. This includes nursing shift notes, doctor visit orders, medication charts, investigation requests, consent forms, fluid balance charts, EMRD checklists, and the final discharge summary.
Together, these records serve three distinct purposes. First, they guide clinical decision-making in real time. Second, they form the evidentiary basis for NABH accreditation compliance. Third, they must now satisfy the structured data requirements of Ayushman Bharat Digital Mission (ABDM).
A paper IPD file cannot reliably serve any of these three purposes — not because paper is inherently bad, but because paper provides no access control, no audit trail, no automation, and no structured data format for digital submission.
| Feature | Paper IPD file | Paperless IPD (PurpleIPD) |
|---|---|---|
| Audit trail | None — changes are untracked | Every edit is timestamped and attributed |
| Access control | Physical access only — anyone with the file | RBAC — role-specific permissions enforced |
| EMRD checklist | Manual — 20–40 minutes per discharge | Auto-populated in real time |
| Addressograph correction | Reprint and relabel every sheet | One-click correction across the entire file |
| Filing errors | Common — wrong sheet in wrong file | Structurally impossible |
| ABDM compliance | Not possible — paper is not ABDM-compliant | Compliant from day one |
| NABH audit readiness | Manual preparation required | Continuous — records are always audit-ready |
Six Real Problems That Paper IPD Creates Every Month
Rather than listing abstract risks, consider the operational problems that paper IPD files create in a typical Indian hospital on a recurring monthly basis.
1. Untracked post-discharge modifications
In a paper IPD file, there is no mechanism preventing a staff member from adding, removing, or altering documentation after a patient has left the hospital. Moreover, there is no way to know this happened. When a NABH inspector queries an amendment to a medication chart or an insurance TPA flags a discrepancy in a consent record, the hospital has no audit trail to reference.
2. Addressograph errors across the entire file
A patient name recorded incorrectly at admission — even a spelling difference — appears on every pre-printed label in the IPD file. Correcting it on paper means physically relabelling every sheet. In a busy ward with a 30-page IPD file, this either takes hours or does not happen completely. Either way, the file goes to the MRD with inconsistent labelling.
3. Manual EMRD checklists consume nursing time
Before every discharge, a nurse or medical officer must manually verify that every required document is present, signed, and complete. In a standard IPD file, this can take 20 to 40 minutes per patient. Consequently, in a 100-bed hospital processing 150 monthly IPD discharges, this single task consumes between 50 and 100 staff-hours every month — hours that could be spent on patient care.
4. Filing and refiling errors reaching the MRD
Paper IPD files get misfiled. Consent forms end up in the wrong patient folder. An investigation report is placed in the wrong slot. These errors are discovered either at the point of discharge — causing delays — or by a NABH inspector during an accreditation audit. For hospitals working toward NABH accreditation, documentation completeness is a scored criterion.
5. Custom labels requiring barcode printer infrastructure
Every time a custom label is needed — for a specific ward requirement, a new form, or a label type not in the pre-printed stock — hospitals must either print from a barcode printer or manage a separate sticker inventory. With a paperless IPD system, custom labels are generated on the fly from the digital record at no additional cost.
6. The doctor bottleneck at discharge
In most hospitals, the treating doctor must physically sign off on the IPD file before discharge can proceed. Given the demands on senior doctors’ time, this creates a bottleneck — patients ready for discharge wait, beds stay occupied, and turnover slows. This bottleneck is a process design problem, not a doctor availability problem.
How RBAC Transforms IPD File Management
Role-based access control (RBAC) is the foundational difference between a paper IPD file and a digital one. It determines not just who can read the file, but who can edit each section, who can lock the record, and critically — who can authorise the final discharge.
In a paperless IPD system like PurpleIPD, RBAC is configured by the hospital administrator to match the hospital’s own operational structure. Therefore, a typical configuration might look like this:
- Doctors — view and edit clinical sections; can review and approve but do not need to be present to close the file
- Nursing staff — access nursing notes, medication charts, and ward-level documentation; cannot modify billing-sensitive or administrative sections
- Medical Officers / Head Nurses — configured to close and lock the IPD file before discharge, eliminating the doctor bottleneck entirely
- Billing staff — view what they need for invoice processing; no access to clinical notes
- MRD / Quality teams — read-only access to archived, locked records for audit and compliance purposes
Once a file is locked by the authorised role, no further edits are possible. The record that existed at the moment of discharge is the record that is archived. This single mechanism eliminates an entire category of compliance risk — the kind that shows up as NABH non-conformances or TPA disputes.
Operational benefit: Configuring file closure to the MO or Head Nurse — rather than requiring the treating doctor — typically reduces average discharge processing time by 30 to 45 minutes per patient in hospitals that make the switch. Across 150 monthly IPD discharges, that is 75 to 112 hours of recovered bed time per month.
This level of access control is one of the defining reasons hospitals evaluating paperless IPD software in India choose a purpose-built solution over attempting to extend their HIMS into the bedside clinical layer.
ABDM Compliance: Why Paper IPD Is a Structural Dead End
Ayushman Bharat Digital Mission (ABDM) is India’s national digital health infrastructure. It requires hospitals to generate structured, linked, shareable digital health records — tied to a patient’s ABHA (Ayushman Bharat Health Account) ID — at the point of care.
This is not a future requirement. Rajasthan has already mandated ABDM compliance for hospitals operating in the state. Other states are following the National Health Authority’s roadmap. Hospitals that delay are building a compliance debt that compounds with every month of paper IPD records.
A scanned PDF of a paper document is not ABDM-compliant. ABDM requires structured data — not images of handwritten notes. Specifically, this means:
- The patient’s ABHA ID must be linked at the point of admission, not retrospectively
- Clinical records must be structured and machine-readable — not free-form handwritten text
- Discharge summaries must be generated in ABDM-compatible formats for submission to the national health data network
- Insurance claims processed through Pradhan Mantri Jan Arogya Yojana (PMJAY) require HCX-integrated documentation, which flows naturally from a digital IPD system
PurpleIPD handles all of this natively:
- ABHA ID is linked at admission.
- Records are structured at source.
- Discharge summaries are ABDM-ready.
Hospitals that implement PurpleIPD are ABDM-compliant from the day they go live — not after a separate compliance project.
The Catalyst HMIS + PurpleIPD Integration: Covering Both Layers Together
For hospitals evaluating how to close both layers simultaneously, Catalyst HMIS and PurpleIPD offer a formal co-sell integration partnership. This means hospitals can implement both the operational HIMS layer and the clinical IPD documentation layer through a coordinated setup — without managing two separate vendor relationships or a custom technical integration project.
What the Catalyst HMIS + PurpleIPD integration delivers
The integration covers the key handoff points between the two layers:
- Admission sync: Patient demographics, insurance details, and bed assignment entered in Catalyst HMIS flow directly into the PurpleIPD record. No duplicate data entry. No risk of name mismatches between systems.
- Real-time bed and ward transfer: When a patient moves from a general ward to ICU — or between any wards — both systems update simultaneously. Clinical documentation and billing records always reflect the patient’s current location.
- RBAC-controlled file closure: The authorised MO or Head Nurse closes the IPD file in PurpleIPD. The locked, complete record is then available to Catalyst HMIS’s billing module.
- ABDM-compliant records: All documentation is linked to the patient’s ABHA ID from admission. Discharge summaries are generated in ABDM-compatible formats through the integrated workflow.
For hospitals currently using Catalyst HMIS: Adding PurpleIPD’s paperless IPD layer closes the clinical documentation gap without replacing or disrupting your existing operational setup. Contact the PurpleIPD team to discuss your specific configuration.
Questions to Ask Any Hospital Management Software Vendor in India
Before finalising any hospital management software shortlist, ask vendors the following questions. These go beyond standard HMS evaluation criteria and specifically test whether a vendor has addressed the IPD documentation layer.
- Does your system handle IPD documentation at the bedside — or is that layer still on paper?
- Is there a complete, tamper-proof audit trail on every edit to an IPD record?
- Can access to different sections of the IPD file be restricted by role — and can the hospital configure who has authority to close and lock the file?
- Is your IPD documentation layer ABDM-compliant? Does it link ABHA IDs at admission and generate structured discharge summaries?
- Does the system automate the EMRD checklist and page count — or does nursing staff still do this manually before each discharge?
- If your HIMS does not cover IPD documentation, which dedicated IPD solution do you integrate with?
If answers to questions 1 through 5 are vague or deflected, you are evaluating a Layer 1 system that has not been designed for the clinical documentation environment. The gap will surface at the next NABH audit or ABDM compliance review. It is easier — and cheaper — to address this during the evaluation stage than after implementation.
Ready to see both layers in action?
Book a 20-minute demo tailored to your hospital’s setup. If you are already on Catalyst HMIS, our team will walk you through exactly how the integration works — and what it takes to go live.
Frequently Asked Questions
What is the best hospital management software in India?
The best paperless IPD software in India is not a standalone product — it is the clinical documentation layer that slots in alongside your HIMS, closing the gap between admission and discharge that every paper-based hospital lives with every day.
What is the difference between HIMS and a paperless IPD system?
A HIMS manages the operational and administrative functions of a hospital — registration, billing, pharmacy, and lab. A paperless IPD system manages the clinical documentation layer: nursing notes, medication charts, consent forms, and EMRD checklists generated at the bedside. Both are necessary. They serve different users and workflows and are designed to integrate, not compete.
Does my HIMS already cover IPD documentation?
Most HIMS platforms include basic IPD modules for billing and bed allocation. However, the full clinical documentation layer — real-time nursing notes, RBAC-controlled file access, automated EMRD checklists, and ABDM-compliant records — is typically outside standard HIMS scope. If your clinical staff still uses paper forms at the bedside, your HIMS does not cover Layer 2.
Can PurpleIPD work with Catalyst HMIS?
Yes. PurpleIPD and Catalyst HMIS have a formal co-sell integration partnership. Patient data flows from Catalyst HMIS into PurpleIPD at admission. Bed and ward transfers sync in real time. Both vendors coordinate the implementation, so the hospital does not need to manage a separate technical integration project. Contact us to learn more.
Is PurpleIPD ABDM compliant?
Yes. PurpleIPD links the patient’s ABHA ID at admission, generates structured discharge summaries for ABDM submission, and supports HCX integration for insurance claim processing. States like Rajasthan have mandated ABDM compliance — and a paper IPD file cannot structurally meet this requirement.
Who can close and lock an IPD file — does it have to be the treating doctor?
No. PurpleIPD uses role-based access control (RBAC), configured by the hospital administrator. File closure authority can be assigned to a Medical Officer or Head Nurse based on the hospital’s structure. This removes the discharge bottleneck without compromising audit integrity. Every closure is logged with a timestamp and attributed to the specific role and user who acted.
Is PurpleIPD suitable for NABH-accredited hospitals?
Yes. PurpleIPD is built specifically for the documentation, audit, and compliance requirements of NABH-accredited hospitals. The audit trail, EMRD checklist automation, and RBAC controls map directly to NABH’s IPD documentation standards. Learn more on the features page.
About PurpleIPD

PurpleIPD is a tablet-based paperless IPD solution built for Indian hospitals by PurpleBits Infosystems Pvt. Ltd., incubated at NASSCOM AI CoE, GIFT City, Gandhinagar. With 20 million+ records digitised across 16 cities, PurpleIPD is India’s dedicated IPD documentation layer — NABH-ready, ABDM-compliant, and integrated with Catalyst HMIS. Learn about us →